Finished notes
Ethan Russo MD - The Endocannabinoid System in Health and Disease
speaking in Sydney, Australia on June 8, 2016 * United in Compassion Medicinal Cannabis Symposium (
United in Compassion)
ethanrusso@comcast.net
Basics:
- Cannabis sativa makes trichomes, which are filled with the essential oil of the plant. This oil includes cannabinoids and terpenoids.
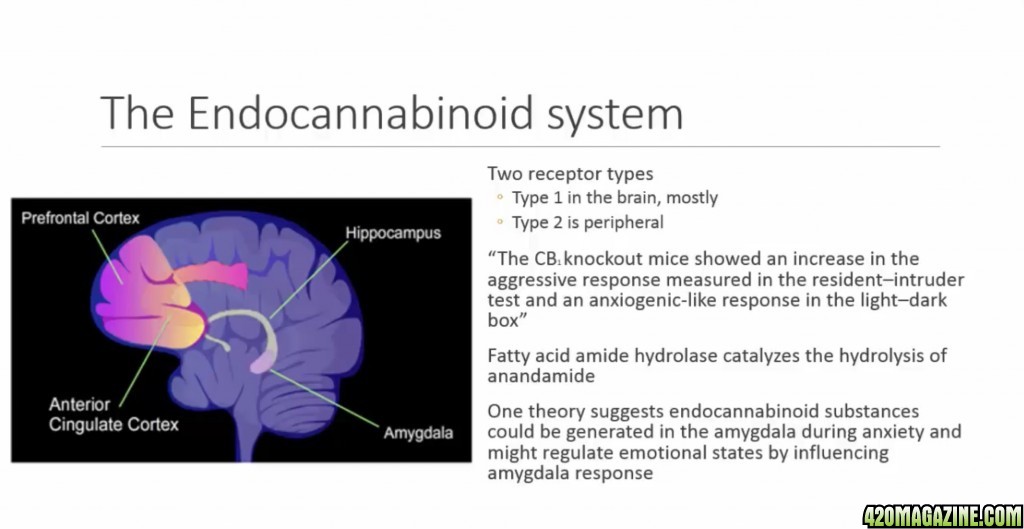
- Cannabinoids bind to the CB receptors found in the body. Most are CB1, and are found in the brain.
- The receptors are like the locks, and cannabinoids are the keys that unlock the receptors.
- Endogenous cannabinoids (anandamide and 2-AG, surely among others, yet to be identified) are those produced by your own body.
- They're created on site and on demand, and bind to the CB1 receptor.
- There are 3 kinds of cannabinoids,
1) phytocannabinoids: basically, 21-carbon items from cannabis, with exception of plants that have Beta-Caryophyllene, which activates the CB2 receptors
2) endocannabinoids: produced by the body
- The ECS has been described as having functions regulating Relaxation Appetite, Sleep, Memory (
I always forget this one 
), and Protection. Rest, Eat, Sleep, Forget, Protect
3) synthetic cannabinoids: some developed before we knew about receptors, some after
- In the brain endogenous cannabinoids act in a retrograde fashion, downregulating the neurotransmitters, originating in the post-synaptic neuron and traveling upstream to attach to CB1 receptors on the other side of the gap. The primary reason for their attachment is to reduce the release of neurotransmitters.
- They're damping down whatever particular function and response that neuron is set for.
- Found throughout the animal kingdom in cordates, animals with a spinal cord
The ECS has three components
1. endocannabinoids
2. cannabinoid receptors: CB1, CB2, and ionitropic cannabinoid receptor (TRPV 1)
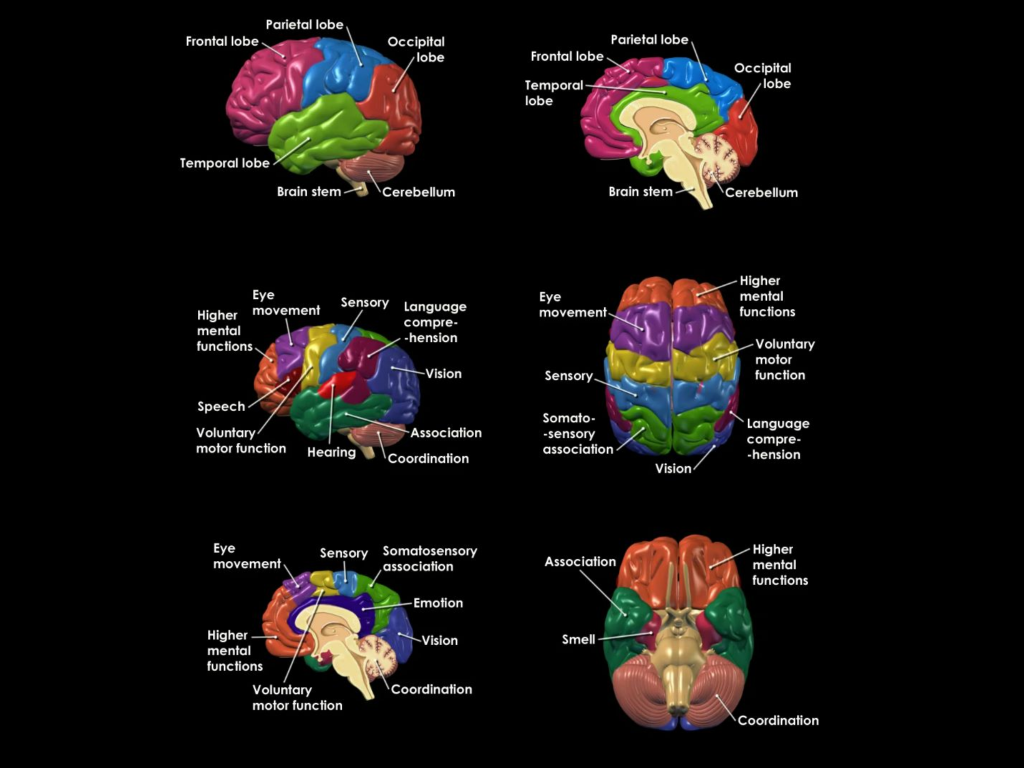
From Medical Jane (highlights are mine): Specialized receptors are located throughout the human body, including but not limited to, in the hippocampus, (memory and learning), the cerebral cortex ( decision making, emotional behavior), the cerebellum (motor control, coordination), putamen (movement, learning), the hypothalamus (appetite, body temperature), and the amygdala (emotions).
When a specific cannabinoid or a combination of cannabinoids bind to a specialized receptor, an event or a series of events, is triggered in the cell, resulting in a change in
- the cell's activity
- its gene regulation and/or the signals that it sends to neighboring cells through the process we call "signal transduction."
3. enzymes that make cannabinoids and break them down;
these can be be manipulated pharmacologically and serve as medicines as well
Entourage Effect
- You have anandamide and 2-AG, but there're also other compounds within the body that, on their own, don't have much power, but working synergistically can deliver a powerful therapeutic punch.
- Soloists and supporting cast.
CB1 receptors in the brain are located heavily in areas that're nociceptive, places having to do with mediating pain
- Additionally found the cerebellum, the limbic system, (emotion), the basal ganglia (movement)
- Receptors are also in reward pathways (addiction and its many effects on the system)
- Receptors aren't found in the areas of the brain having to do with respiration, so cannabinoids can't kill you like all the wonder drugs can. This is how opioids kill.

They depress the respiratory center of the brain and your body forgets to breathe.
The cannabinoids also work in the spinal cord, in the periphery, and in the gut.
- CB1 is the most prolific CB G-protein receptor
in the brain, where it modulates the release of neurotransmitters.
- Glutamate is typically overactive in neuropathic pain. If cannabinoids damp down glutamate response, that would effect pain over time.
- Modulates pain, memory, movement, whether someone will vomit or not, their seizure threshold.
- Also modulate many other body systems, incl. the gut.
The brain and the gut speak for themselves same language.
- Cannabinoids mo
- propulsion: the speed with which things move through the gut
- secretion: how much liquid or lack of liquid is brought into play during digestion and elimination
- One of the first successful treatments for cholera (major symptom is deadly diarrhea) in the 19th century was cannabis.
If we think of CB1 as the psychoactive receptor we then look at CB2 receptors, found mainly in the periphery, as pain and inflammation.
- Drugs that could effect only CB2 receptors wouldn't have any euphoric effect.
- Such drugs could be promising in treating fibrotic diseases like scarring in the liver or other organs.
Both kinds of receptors are found in the skin.
- Exciting therapeutically due to accessibility (don't need to go through a lot of layers to be active)
- Currently an area of intense research.
CBD, which doesn't attach to either receptor with any real affinity seems to be a valuable cannabinoid for the skin.
- A full-spectrum cannabis extract with CBD would show antibacterial effects (as in acne).
- CBD works on TRPV-4 receptors, which reduces the release of fat (sebum), which contribute to acne.
se·bum
ˈsēbəm/
noun
an oily secretion of the sebaceous glands.
Sebum Definition - Verywell
Apr 15, 2017 - Sebum is a light yellow, oily substance that is secreted by the sebaceous glands that help keep the skin and hair moisturized. Sebum is made up of triglycerides, free fatty acids, wax esters, squalene, cholesterol esters, and cholesterol. ... It also includes lipids from skin cells, sweat, and environmental matter
CBD was recently shown to stimulate bone fracture healing.
- Right now cannabinoids are banned from professional and amateur sports. It might be time to rethink that. Cannabidiol will speed the healing, without side effects.
Cannabis will accelerate the heart rate.
- Interestingly, at a higher dose it will slow the heart rate down, far enough to make it difficult to regulate blood pressure.
- You can pass out from orthostatic hypertension.
Concerns:
- There was a rise in concern that cannabis might contribute to heart attack, but the thinking is the signalling isn't strong enough to make this drastic an effect. It may be a concern for individual patients, but not as a population concern.
- For a time there was concern that there might be an arthritic response to cannabis. Upon closer inspection it was discovered that the patients were all tobacco smokers, and tobacco is known to constrict blood vessels in the hands (Berger's Disease).
The most common use of cannabis is for the treatment of chronic pain conditions. Cannabis offers relief through various pathways
- Through neurotransmitters
- through interaction with opioids, whether by pill form or the endogenous opioid system
- direct effects in the brain
- other components in cannabis beyond the major cannabinoids, CBD and THC
The brain has a base-line level of cannabinoid function (the endocannabinoid tone)
- Under certain conditions activity can be either depressed or enhanced.
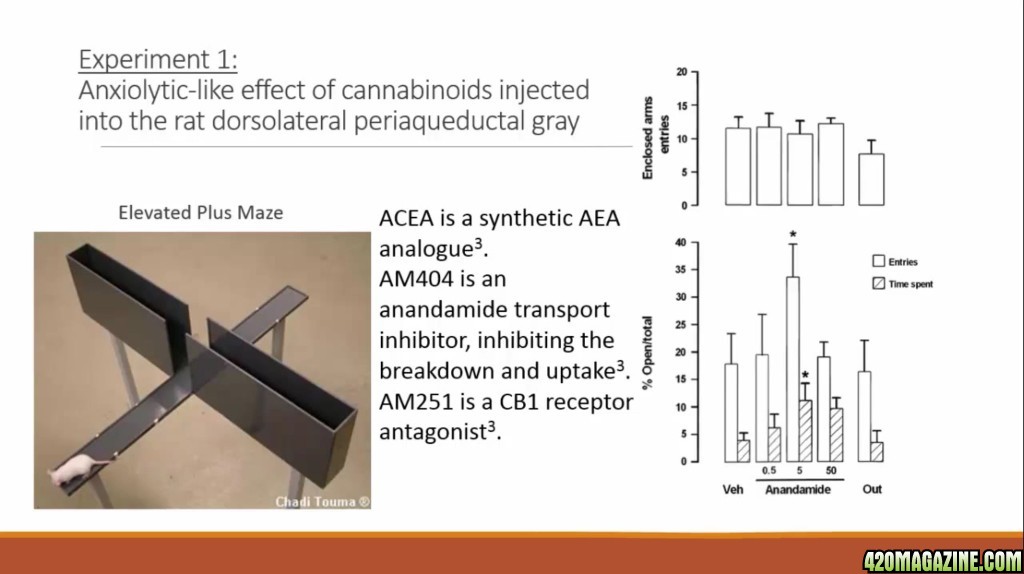
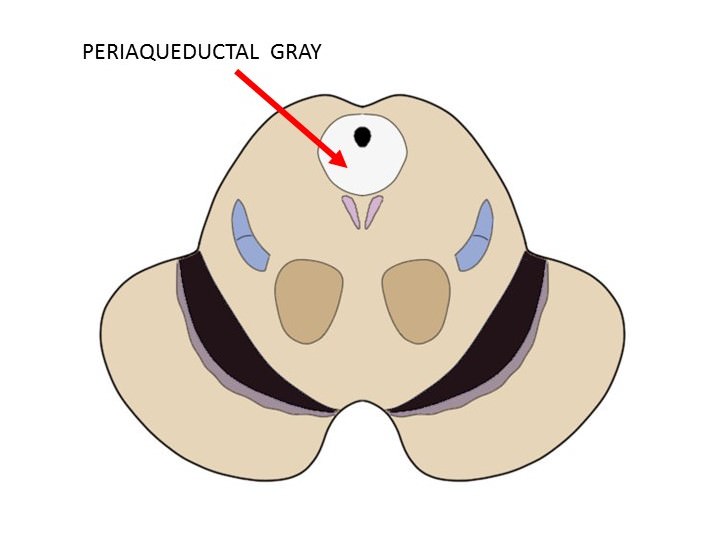
- the periaqueductal gray is a mind brain generator (???)
The periaqueductal gray, or PAG, is an area of gray matter found in the midbrain. The PAG surrounds the cerebral aqueduct (hence the name periaqueductal) and occupies a column of brainstem that stretches about 14 mm long. There are no obvious visible anatomical divisions within the PAG, but researchers have divided the PAG into four columns based on differences in connectivity and function: the dorsomedial, dorsolateral, lateral, and ventrolateral columns.
What is the periaqueductal gray and what does it do?
Although the functions of the PAG are complex and not fully understood, since the 1970s it has best been known for its role in the inhibition of pain. Indeed, some have argued that its identification as an "analgesia center" has hindered a more complete understanding of the functions of the PAG. An increasingly intricate appreciation of PAG function, however, has been emerging over the past few decades
When the PAG was first found to have an association with pain, it was observed as playing a role in pain transmission---or the sending of pain signals to the cortex---and not the mitigation of those signals. Eventually, the PAG would come to be much better recognized as an area important to pain inhibition. In the late 1960s, the first indication of the role of the PAG in pain suppression emerged from a study that found that stimulation of the PAG in rats allowed researchers to perform surgery on the rats without the use of anesthetics (and without the animals exhibiting signs of severe pain). Further studies found that PAG activation was associated with the inhibition of spinal cord neurons involved in pain signaling. By the mid-1970s, stimulation of the PAG was already being used as an experimental approach to treating chronic pain in human patients. The fact that some of these experiments reported success in the treatment of chronic pain supported the role of the PAG in analgesia. The patients involved in these experiments also often complained of a wide range of side effects linked to PAG stimulation, however, suggesting that many more functions than analgesia were connected to the PAG.
- Cannabinoids also active in the thalamus (ventral postural lateral nucleus). Tested in this area cannabinoids are 10 times more powerful than morphine. It becomes obvious that using the two drugs together would be a beneficial approach for pain management.
- There are additional functions in the spinal cord by which cannabinoids effect pain levels and perception.
Cannabinoids can be effective against contact dermatitis (poison ivy or plain old itching)
There are numerous randomized trials on cannabis and pain. The problem is that the company that holds the rights to market isn't choosing to do so in many markets.
Just exactly what we anticipated. Give Big Pharma control and they won't market something they can't make the big money on. Keep this plant out of their hands and in the control of the people.
An interesting thing occurred when they tested cannabis with cancer pain in hospice settings. The patients got relief and the tolerance levels didn't rise in the same way they see with opioids. There wasn't the standard increase in pain levels with cannabis or Sativex.
- The gold standard in pain is the group that has a 30% reduction in pain over time.
- In the study 43% of patients using Sativex got relief, as opposed to 21% with the placebo.
- The study contrasted placebo, Sativex and a full THC isolate extraction. The isolate didn't work any better than the placebo. The Sativex, with its inclusion of CBD, did work, and in dramatic fashion.
- This was the first concrete evidence of th entourage effect in pain control.
Placebos work
Faith is a powerful tool, and I'm convinced the ECS can heal a disease-wracked body instantaneously, so the placebo effect doesn't surprise me in the slightest.
- Have a placebo that works so well and you'll end up with your effective drug looking ineffective next to the placebo, making your drug look statistically insignificant.
In a randomized withdrawal study of Nabixinol,Sativex, and MS patients were unknowingly started on Sativex at either a level to control spacisity or to keep them from having too many side effects.
- The 20% who improved were brought back and then randomly half were refilled with placebos.
- All patients who stayed on Sativex improved spacisity, and all patients on the placebo went into decline.
- These results were the impetus for gaining approval for Sativex administration in 27 countries.
Are we one of those lucky countries?
- They had patients with twisted limbs that had the muscles relax after administration of Sativex
I believe Sayivex is a balanced ratio medication.
Clinical Endocannabinoid Deficiency
- Your endocannabinoid tone is an indicator of the number of cannabinoids available, how their produced and degraded, and how many receptors you have available.
- A change to any of those areas can effect the endocannabinoid tone, resulting in pain, stiffness in the muscles, the seizure threshold, etc.
- The theory was that in certain conditions if the tone is depressed too low it'll produce disease and symptoms in the system.
- In original 2004 paper he focused on migraine, fibromyalgia and IBS. All three are hyper analgesic responses, where the system has a heightened pain response.
- All three are difficult, if not impossible to track or determine by lab testing, so they're diagnosed based on clinical determination of the patient's described patterns.
- They're all also comorbid, meaning if you have one, you likely have the other two. Primary headache turned up in 97% of the cases with fibromyalgia. 33% of patients with chronic daily headaches (a type of migraine) also had fibromyalgia. 32% of patients with IBS had fibromyalgia and 32% of fibromyalgia patients also had IBS.
Unfortunately, these conditions show up in large numbers of women who get misdiagnosed as being psychosomatic by their male doctors.
- Russo maintains that this is a biochemical disorder, possibly due to a drop in endocannabinoid expression, and there's no mind game these women are playing with themselves.
IBS: Sometimes thought of as a life-long condition, but people clearly acquire this at some point.
- It's the most frequent diagnosis among gastroenterologist in the states.
- There are no particular regular signs, but there is a pattern of irregular bowel movements, often diarrhea, although this could be constipation. They can alternate too.
- It's being described as a disorder of unknown origin and treated by agents of an unknown mechanism of action.
- There are many ineffective drugs. The target should be the ECS instead.
- IBS brings the joy of visceral hypersensitivity. Things hurt, and hurt bad. Again, an over abundance of pain.
- It's known that anandamide works with colonergic neurons, the primary movers of the gut. It performs a modulatory role on the speed of digestion and elimination.
- The ECS appears to be unregulated in diseases of the gut with inflammation. This would be true in the case of IBS as well.
The Mayo clinic, looking at genetic markers of IBS, found CNRI (has to do with cannabinoid function)
- Patients with IBS responded positively to THC.
- CB1 receptors seem to modify the speed through the gut.
Relationships to diet
- If you eat the right things you might not have to use cannabis so much.
- Replenishing the gut flora with probiotics enhanced pain management. They positively effect the RNA expression of the gene associated with CB receptors when taken as a supplement.
- This enhanced the pain control function of morphine.
- It was proposed that taking a CB2 antagonist would enhance that function.
- 32 out of 45 studies on the addition of probiotics showed an improvement in gut performance and health for patients with IBS, incl. less pain, less bloating, etc...
- 5-6 months of continuious supplementation created a stable environment in the gut.
A recent study found that THC alters the bacterial presence in the gut.
- In these mice that had a predisposition to being obese, the THC prevented weight gain through the action of changing the balance of the gut bacteria.
Prebiotics, vegetable matter that feed the good gut flora. (FOS) They don't get broken down in the stomach and they're fermented by the gut flora.
- There are over a thousand different species of bacteria being brewed.
- Prebiotocs help the healthy, beneficial gut flora grow and prosper.
- It's estimated that ancient man ate a lot more of these valuable vegetables. Modern humans may only get a few grams a day.
- Best sources acacia fiber, gum arabic, chicory, burdock, sunchokes (Jerusalem artichoke), onions, leek, garlic, dandelion greens,
- They reduce infectious diarrhea, alleviate inflammatory bowel diseases, reduce cancer risk in the gut, increase mineral absorbtion, lower cardiac risk, and decrease obesity.
- 10 grams a day - a heaping tablespoon of acacia fiber that could be added to any number of foods, increased lactobacillus sixfold and increased balance of the gut flora. It also appears to decrease the bug that causes c-diff.
All of this information on the gut is in a recently published article (published last May or June).
Fibromyalgia
- German study looked at nine patients of fibromyalgia, taking up to 15 mg of THC daily.
- It was a THC isolate, and too strong an experience for 5 of the 9, who dropped out of the study.
- The remaining 4 patients saw relief, a decrease in Allodynia (extremely painful touch), or Hyperalgesia (hyper sensitivity to pain).
- Also saw a sipratistically significant reduction in pain overall. Statistically, this should only happen in 1 out of 100 patients, and yet all four saw this improvement.
Nabilone is a THC semi-synthetic marketed in some countries.
- It's about 10x the potency of THC. Not really therapeutically useful except in the most extreme cases, and even then.....
- Study tracked 40 patients that got one dose a day equivalent to 20 mg of THC, a fairly high dose.
- After four weeks a review of a visual analog scale (where patient judges their pain on a numeric scale), the Fibromyalgia Impact Questionaire, and anxiety levels.
- Improvement was statistically significant across the board.
- Regardless, not a drug that patients can take over the long run with any success.
Mark Ware in Canadian study contrasted Nabilone compared to Amotriptoline (?), a commonly prescribe bed drug for fibromyalgia, looking at sleep.
- 100% of fibromyalgia patients suffer from sleep disturbance. Patients won't improve until sleep is restored.
- In this study sleep was improved, but there was no significant reduction in pain.
A Spanish study of smoked cannabis was only done acutely, looking at pain, stiffness, relaxation, sleepiness, and wellbeing.
- 28 patients with cannabis, 28 controls.
- Within 2 hours, many parameters were statistically improved.
- Mental health component was also higher in the group that recieved cannabis, meaning they had psychoactive side effects.
- It's almost a given that it was a high THC variety used in this study, with no Cannabidiol because that was what was available at the time of the study.
National Pain Report looked at 1300 patients with fibromyalgia and asked for their benefits from taking 3 FDA-approved drugs commonly prescribed for fibromyalgia, contrasted with cannabis.
- The Pharma drugs were basically ineffective.
- Over 60% of cannabis-using patients claimed a really good result and found cannabis effective. Only 5% had no benefit with cannabis.
- Which is the best choice? Hands down cannabis.
Migraine
- For a common affliction migraine is probably the most biochemically complex malady people suffer.
Study of women with migraine looked at the anandamide membrane transporter and the activity of FAAH (enzyme that degrades anandamide).
- Looking at platelets in the blood (brain tissue isn't ethical in living patients

).
- Compared patients with chronic headaches vs controls.
- Levels of CB1 receptors were equivalent in the two groups, but women with migraine had an increased degradation rate of anandamide, and decreased platelet levels that could indicate an ECS deficiency that was contributing to the migraine.
Airman et al did a series of studies looking at ECS function in migraine.
- One of the things that migraine does is make blood vessels too big or too small. Not the cause of the disease, just an epiphenomonen, a secondary effect.
- Anandamide reduced blood vessel diameter in the dura ( the protective cover of the brain) by 30%, through a complex biochemical mechanism.
- It was felt that anandamide maintains a base level in the brain (a tonic level of activity).
- Anandamide modifies the trigeminalvascular system, the path of physiological mechanism in migraines.
Another study of the vascular system showed the involvement of TRRP-V1 set of eCB receptors.
- Used a synthetic cannabinoid, looking at synaptic activity.
- Study suggested that CB1 antagonists like THC have therapeutic promise in migraine and cluster headaches.
- Authors were fearful of the psychoactive side effects.
- Overlooks the fact that a very low dose, that isn't psychoactive is sufficient to treat these disorders, or that you can temper the euphoria with the inclusion of Cannabidiol or terpenoids.
Probable the best evidence of clinical eCB deficiency is a study proposed in 2004 but carried out later by the Italians.
- He suggested that looking at cerebral spinal fluid for levels of eCB in patients with migraines.
- It requires a spinal tap, something the ethics committees in the US would be adverse to allow.
- The Italian researchers looked at normal levels (it's unknown how they convinced the patients to do a spinal tap - maybe ethics weren't the big concern in Italy) in control group, contrasted by patients with migraines.
- Only a 1 in 10,000 possibility that the results were by chance.
- Author said "Reduced eCB levels in the cerebral spinal fluid of chronic migraine sufferers support the hypothesis of the failure of the ECS in chronic migraine.
- This proves the existence of clinical eCB deficiency.
In another Italian study, both anandamide and 2-AG markers were dramatically reduced in the platelets of chronic migraine patients as compared to controls.
- Very highly statistically significant.
In another Italian study an animal model of migraine is explored.
-Migraine creates some bizarre symptoms, like the loss of vision on one side with bursts of light (sparkles), caused by a depression on the surface of the brain.
- The study showed the involvement of the ECS. Theoretically, THC could prevent or stop the progression of this effect.
- Many patients report that cannabis is used at the onset of the array it will prevent the symptom from becoming full-blown.
There's a genetic predisposition to migraine.
- It's been mapped to CNR1, an eCB gene, on chromosome 6.
- Patients with the strongest evidence for this gene also had the highest likelihood of having symptoms like sensitivity to light, nausea, and significant disability with their headaches.
- Patients with strongest evidence of CNR1 also showed neuroticism, depression, and a tendency towards drug dependence. (Someone with mirgraines will obviously be trying to treat it with one substance or another.)
Study out of Colorado in mid 2016 looked at 120 patients with migraine using cannabis to prevent or control migraine.
- Patients were treated prophylactically to prevent migraine.
- 60% of patients had used cannabis previously.
- Of those who went on to use cannabis regularly dropped the occurance rate from 10.4 a month to 4.6 a month, very statistically significant.
- Also reduced headache frequency and were able to abort, or stop their headaches when cannabis was used acutely.
- It's a selective population. The same thing needs to be done in randomized, controlled trials. Russo has been unsuccessfully trying to get those trials to happen for over 20 years.
John McPartland wrote "The Care and Feeding of the ECS."
Care and Feeding of the Endocannabinoid System: A Systematic Review of Potential Clinical Interventions that Upregulate the Endocannabinoid System
- Looked at issue of the eCB deficiency
Where do we go from here?
- We need better studies of IBS, Fibromyalgia, and migraine, looking for levels in the blood, levels in the cerebral spinal fluid.
- It'd be better to do this with scans of the brain, but for right now we don't have great tools this way.
- There's active research, but it'd be nice to be able to assess the eCB function or eCB density in the brain without having a needle stuck into your back.
- We need better work genetically. There are companies looking for markers of these diseases and trying to coordinate them with eCB function.
- Controlled clinical trials of cannabis-based medicines in these clinical conditions are what will convince physicians and politicians.
"Only time and the scientific method will ascertain whether a new paradigm is applicable to human physiology and the treatment of its derangements. Our insight into these possibilities is dependent on the contribution of one unique healing plant. For clinical cannabis has become a therapeutic compass to what modern medicine fails to cure."
Cannabis modulates the ECS, which is, in itself, an innate homeostatic regulator of human physiology. If there's too much of something, it brings it back down into balance. It there's too little of something, it brings it up into balance.
- Cannabidiol is a particularly interesting cannabinoid system modulator.
- In future we may see more CBD with only a little THC.
- The ECS is influenced by lifestyle and dietary factors.
- Primary beneficial approaches would be low-impact exercises, an antioxidant, anti-inflammatory diet, probiotics and probiotics. Of of these will improve the conditions discussed.