Medical Cannabis Treatment for Adults and Children - Dr. Bonnie Goldstein
United in Compassion Medical Cannabis Symposium, Sydney, Australia, June 14-15, 2016
We need to stop identifying cannabis as a drug of abuse. It's a medicine.
- In all her years working in pediatric ERs with over 60,000 patients she never saw a cannabis patient problem.
- No one has ever died from ingesting cannabis.
- Education is the only way to move the message forward. Educate ourselves and share that knowledge.
In her practice she sees both adult and pediatric patients.
- Pediatric patients are mostly confined to treatment-resistant epilepsy, autism, and advanced cancer, though she does have some psychiatric disorder patients.
- Beginning to see an increase in a newly-diagnosed and little understood PAD or PANDA, a type of Pediatric Autoimmune Disease.
- The most common thing they see adults for is chronic pain, followed by a long list of everything, including sleep disorders, psychiatric concerns, and so on.
- Because of where the receptors are located the ECS effects almost every physiological system in the body.
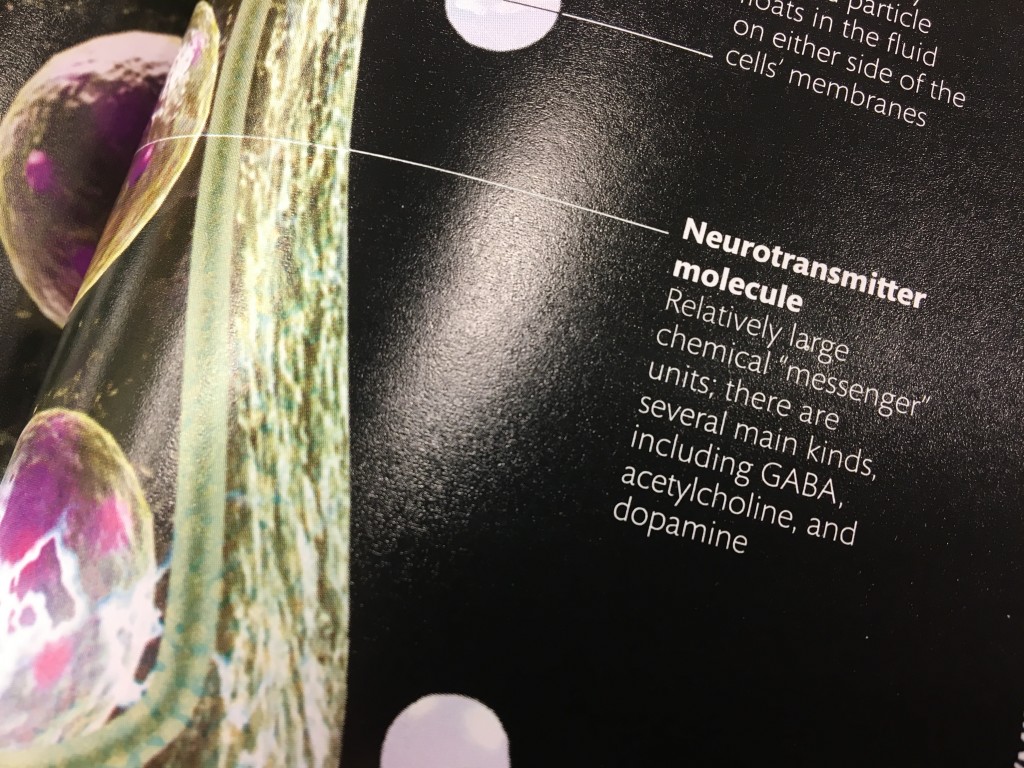
There are over 400 compunds in the typical cannabis plant, over 100 of which are cannabinoids, the most studied among them THC and CBD.
- It's going to work differently in the body than a single isolate med will.
- Breeders are beginning to develop designer strains with increased amounts of particular cannabinoids.
- The entourage effect: the sum is greater than its parts. Choose whole-plant medicines and full-plant extractions over isolates.
- Terpinoids are basically essential oils that have medicinal properties.
The choice of what strain to choose to treat a particular disease is entirely individual.
- Determine the patient's goals from the treatment and assess the general condition of the patient.
- How is the patient expressing the disease? What's the underlying cause and how is this disease expressing itself in this patient.
- You want to pursue an individualized approach. Cannabis will offer an individual response.
- Patients with identical diagnoses, using identical strains with th same cannabinoid and terpene profiles and at the same dose, and have completely different response and experiences.
Start low, go slow
- Begin sub-therapeutically and titrate up slowly and thoughtfully.
- Dr. Abrams of UCSF stated it as "Patient will determine self-titrating dose."
- Its a little different for epileptic and cancer patients, but generally the patient gets to choose the dose.
- You'll find the sweet spot by trial and error, titrating up until you feel "too much!!" and then backing off one increment. This is the optimal therapeutic dose.
I like the way Martin Lee expresses it: you want a CBD-rich medication with as much THC as the patient can tolerate.
Cannabis is
not one size fits all.
Your endocannabinoid tone is of great importance. Fall below or above that baseline and disease comes calling.
- She explains it to her patients as you have a point of balance where your ECS is working well. Disease sets in if your tone becomes deficient. Over-excitability of the system leads to receptors being taken off line, which can complicate things too.
- She likens it to a thyroid condition. If the thyroid was deficient your doctor would prescribe thyroid medication. If the ECS is deficient you bring in more cannabinoids, terpenes, and flavonoids.
- If you or someone you love has disease you haven't found a pharmacological solution to its worth supporting the ECS.
- If you're not supporting the ECS you're shooting around the target when the ECS is the bullseye.
New patient intakes include
- history, what they've tried as treatment, whether or not they've used cannabis before
- A cannabis naïve patient or one who used slightly years ago need to be handled differently from experienced patients.
- If someone used years ago you want to know what they're experience was like to help you decide which strain to choose and what treatment path to take.
- For someone who remembers being stressed by the experience, this may suggest they have a sensitivity to high THC or sativas.
Delivery method needs to be properly matched to the patient.
- Ask the patient "What sounds good to you?" (Speaking of experience)
- A patient going through chemotherapy may not be able to process edibles in the way you need. Chemo destroys the gut flora, so things don't get absorbed.
How frustrating would that be? 
- There must be options for delivery methods so patients have a wide range to search through to find what works for them.
- A majority of patients us inhalation (smoking or vaping), sublingual tinctures, and a small percentage of patients find edibles help.
- Dosing through the liver can be trickier with metabolism.
Effects of THC and CBD
- With most patients a combination formulation works best.
Bonnie's 3-Tier approach, developed so that patients would be able to read labels and determine the anticipated effects of the different ratios.
1) THC-rich medications are strong in the THC effect.
- The thought that THC is only recreational is erroneous. THC is powerful medicine. Control it with dosing and delivery.
- Don't drive when you're intoxicated
- Patients use THC-rich meds to treat sleep, pain, nausea, mood and appetite.
2) High ratio CBD:THC will be mostly influenced by CBD.
- This offers meds for daytime that avoids euphoric effects that come with THC.
- It's not sedating
- choose this type if treating pain inflammation, mood, and seizure disorders.
- Patients usually see euphoria fall away at 10:1.
3) Low ratio CBD:THC will have some intoxication, depending on the CBD content and the terpene profile.
- May or may not be psychoactive, it's that individual response, determined by patient's condition, how experienced a cannabis consumer they are and how their brain responds to the cannabinoids.
- CBD will buffer some of the euphoria, depending on your system's response to the compounds.
- Patients find relief for pain, inflammation, mood, sleep, neuropathic pain, and nausea.
Case report: 54-yr old woman with diabetic neuropathy.
- Middle school counselor, so very private about her cannabis use.
- History of adult-onset Diabetes 2 with 6 years of nerve pain interfering with sleep.
- Used to be morbidly obese, and underwent gastric bypass. Glucose was controlled by the procedure, but neuropathic pain persisted.
- Tried numerous drugs, including Gabapentin and opiods, to no avail.
- A friend gave her a cannabis edible prior to her visit, probably a high THC product, and she had complete relief from pain and was able to sleep again. She visited Dr. G to become legal.
- Started her on high-CBD tincture (25:1) for pain and uses topicals for feet if bothering her.
- She only treats on days when she has pain.
This seems counterproductive to me. Obviously a baseline of available cannabinoids would go a long way to promoting more healing.
- At bedtime she uses a 1:1 ratio edible. She takes it at about 8-9 PM and gets between 618 hours of uninterrupted sleep, and her feet don't hurt when she wakes up in the morning.
- Again, if no pain she passes on the dose. She says some weeks are good, some not so good.
- She's now off all pain and sleep medications. She is now controlling with diet and is pharmaceutical-free.
Case report: 26-yr old woman with juvenile rheumatoid arthritis, diagnosed at the age of 15.
- Dr. G saw her first at the age of 24.
- Patient had significant side effects with conventional medication. She'd had a life-threatening reaction to one medication that sent her to the ICU, and she sought out Dr. G following that event.
- She was wheelchair bound, severely depressed, with severe pain and swelling, unable to go to school and care for herself.
- She was the oldest of four sisters, and the other two were living normal lives. She was feeling left behind, which caused anxiety and depression.
- She started out anti-cannabis, but enough friends and family had suggested it that she wanted to at least try.
- Started on a high-dose CBD oil, at a ratio of 27:1, upwards to 200 MG of CBD per day in three doses, spaced 8 hours apart. Also uses high THC sublingual meds for breakthrough pain.
- She knew she was getting better can now clip her own fingernails. She started cooking and can now shower on her own.
- She isn't taking any other medications
Case report: 47-yr old man, a construction worker, father of two, who had a severe work injury to his spine that herniated lumbar disc.
- Went the typical pharma route of opioids, muscle relaxers, nonsteroidals, physical therapy and epidural injections, with no real relief from any of that.
- He was reluctant to have surgery. From a family of police officers, he was reluctant to enquirer about cannabis, but someone had started him on cannabis, it worked, and he wanted to be legal.
- CBD was ineffective for his pain. He uses THC-rich meds at night.
- He says if he's overexerted himself at work and feels inflammation flaring up he now uses CBD as well at night, and he found he doesn't get the full-blown episodes where he can't get out of bed.
- He uses acupuncture and exercise to assist healing and is now pharmaceutical-free.
Pediatric use
- Science is pointing to ECS deficiency with seizure disorders and autism. If it's the ECS that's failing, it's the ECS we need to treat.
- Cannabis has an excellent safety profile. She sees no negative side effects with any of her pediatric patients.
- Quality of life is everything for these families. It may not be the perfect solution, but there usually will be some improvement and no negative side effects.
- Compassionate care and end-of-life patients.
- It took California nearly 22 years after passing the first MMJ law to finally get regulations up and running.
CBD use with epilepsy
There were 3 small trials with CBD and pediatric patients in the 70s and 80s. The last of the early trials with CBD and epilepsy was in 1985, and nothing else was done until 2005.
Findings showed
- CBD was well-tolerated
- there were little to no side effects
- it was a promising therapy
A 2005 presentation to the 2005 Congress on Cannabis and Cannabinoids in The Netherlands, summarizing an open study of 18 patients with refractory seizure disorder
- no side effects requiring CBD discontinuation
- the majority of patients saw at least a 25% improvement in seizures with low CBD doses
- all patients recieving CBD had improvement in consciousness and reduction in spasticity, if that was a symptom
Report in
Epilepsy and Behavior in 2013
- 2 Stanford doctors interviewed 19 patients with severe epilepsy using CBD-rich cannabis (using Charlotte's Web)
- The average number of anti-seizure medications used was 12.
* Only 50% of children respond to the first medication used.
* Percentages drop with each new drug introduced- 13% respond to the second medication, 1-4% respond to the third medication.
* If you're trying 12 medications you can be sure you have a treatment-resistant condition, at least which conventional treatment.
THIS IS PURE BULLSHIT!!! To put children through this is reprehensible. I don't believe in hell, but there are moments I wish I did.
In their survey they found that 16 out of the 19 families reported a reduction in child seizure frequency while using Charlotte's Web.
- Two of the children became seizure-free.
These were children who'd been told they were intractable.
- 8 out of the 19 reported a greater than 80% reduction.
- 6 out of 19 reported a 25% - 60% reduction
Beneficial side effects
* Increased alertness
* Better mood.
* Better sleep.
Adverse side-effects
* drowsiness
* fatigue
A small study out of Colorado showed that 73% of patients that took CBD oil showed a 98 - 100% reduction in seizures.
- At 3 months 45% were seizure-free
At 34:00 she begins to explain a chart we can't see in the video that would be really nice to find. It shows drug interactions with CBD.
- CBD can be metabolized in the liver, where many of these other drugs are also metabolized.
- Clobazam (brand name - Onfi) levels skyrocket upon administration of CBD. In one patient it rose to over 400%, where for others it was as low as 70 - 80%.
- The medication cocktail that the patient is on can confuse all the variables.
When adding CBD to the regimen of a child on Omfi you know to watch out for side effects, because Omfi levels aren't something anyone's thinking to check.
When adding CBD to a regimen that includes Lamotrigine (brand name Lamictal) alert the parents that an increase in seizures isn't the CBD, it's because the CBD is causing the Lamictal levels to drop, and because the practice is to start low and increase slowly there may not be enough CBD in the system to pick up the slack.
In a survey in UCCA of 117 families using whole plant oils to treat their children's seizure disorders:
* 85% reported seizure reduction
* 14% reported complete seizure reduction
* average number of anti-seizure meds was 8
Reported benefits
53% - improved sleep
71% - improved alertness
63% - improved mood
The study listed increased appetite as a bad side effect, but this is a disconnect from the reality the families share. Most families are pleased to have their children take an interest in food.
One study found that using CBD with Clobazam increased the chances of having seizure reduction
Clobazam co-therapy was associated with a higher rate of treatment - 57% vs 39%
*** You can use them together to get the dose of Clobazam down to a level where the negative side effects fall away.
She has two patients that they weaned entirely off pharmaceuticals that had seizure reduction, but not cessation. Once pharma drugs were gone there was a slight rise in seizures, so they put them each on very low dose Omfi and the children stabilized with reduced seizures.
Combination therapies are possible with patients with therapy-resistant conditions.
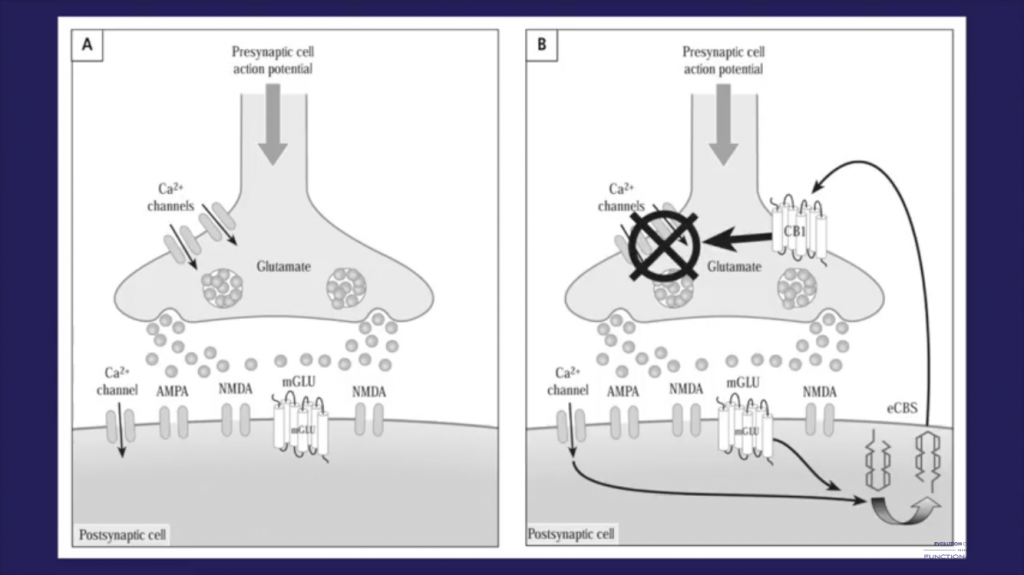
How CBD Works As An Anticonvulsant
THC is monogamous to the CB1 receptor
CBD has multiple sites of action.

- receptor-independant channels
- binds or blocks to 9 eCBRs
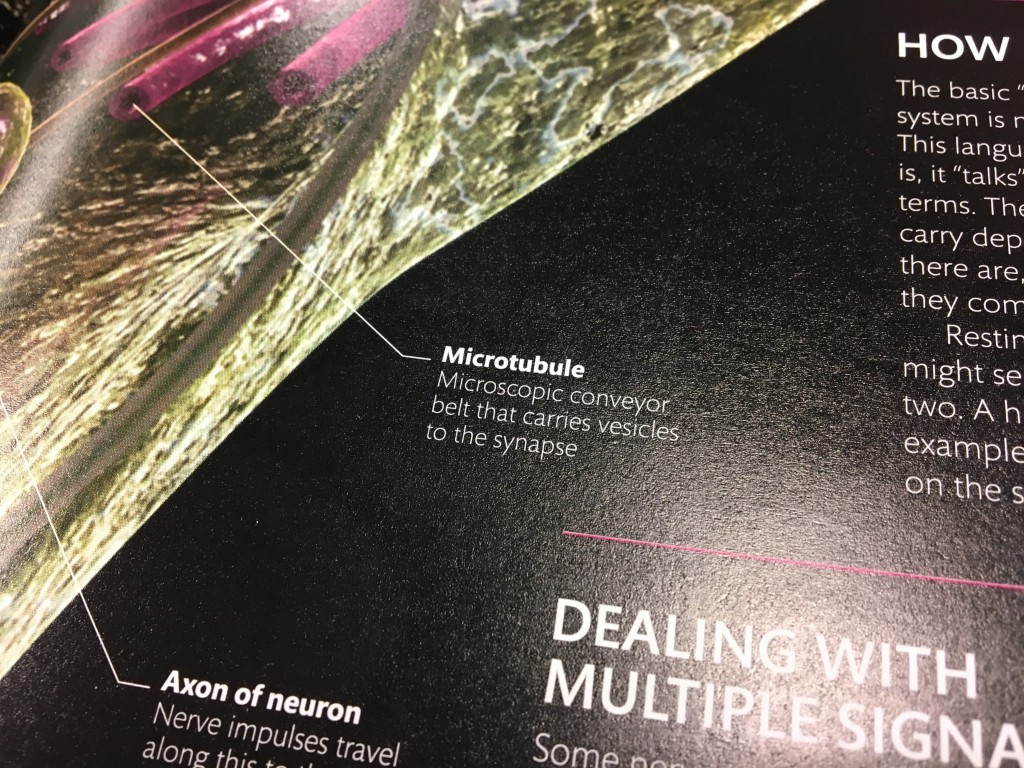
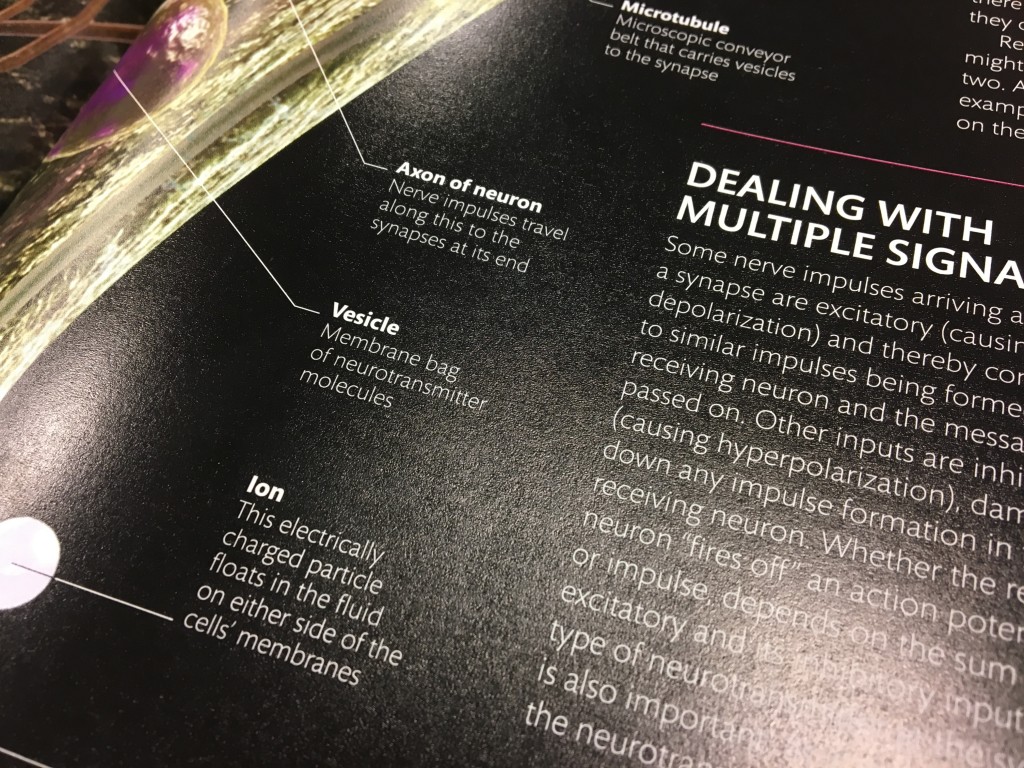
- modulates the flow of neurotransmitter
- modulates calcium channels
- CBD will block the uptake of your own endocannabinoids. If the child is having seizures due to an Endocannabinoid deficiency, CBD can theoretically enhance the child's ECS by freeing up anandamide.
- anti-inflammatory
- neuroprotective
- anti-oxidant
CBD is a multi-tasker, working on many levels and from many pathways. This may explain the widespread success with epileptic patients.
The challenge of tolerance
Patients with severe seizure disorders can develop tolerance, and you really can't keep ramping up the dose without introducing unwanted side-effects.
There's some concern about the effects of euphoria on the developing brain.
I don't know if this is justified. There's anandamide in breast milk. It's my understanding that young children don't have the same concentration of eCB receptors as adults.
- We don't know the long-term effects of the multiple anti-convulsants on my the developing brain either. Cannabis looks like the better choice here.
Clinically she's found low doses of THC, either sub-lingually or through the gut, can be very helpful when weaning off anti-convulsants.
- If you're getting good results with co-therapy and decide to wean off the pharma drugs you may see an increase in seizures, called "withdrawal seizures". Families report that if they use low-dose THC for a couple weeks following a step-down reduction it can help them get through a very difficult period.
If you can get oil to 10 mg of THC per 1 ml, you can load a 1 ml syringe and administer down to .1 ml. Some children are very sensitive to low THC doses. You don't need a lot.
.1 ml is equal to about four drops, or 1 mg of THC in this particular formulation.
Doctors are enamoured with controlled dose.  I see their point and counter that with cannabis "Close enough for government work" will also get the job done without dangerous side effects.
I see their point and counter that with cannabis "Close enough for government work" will also get the job done without dangerous side effects.
- You can titrate slowly and find the sweet spot, and then repeat it when you use oils you know the cannabinoid count in. [COLOR="#80008
She starts with a 25:1 or 27:1 CBD:THC ratio.
Most of her patients are using either Charlotte's Web or AC/DC. There are now 8 different chemovars that meet the requirements for effective medication for seizures.
Find out what they are.
- If one doesn't work, try another.
She recounts the story of a young patient who developed rage following brain surgery. They have him on a 10:1 ratio, using a high THC medication. His seizures are under control (from 50 grand mal a month to 6) and he's back in school.
Having more than one chemovar means you can custom-mix a formulation that works for this particular patient.
- If you're trying strain after strain and not finding relief, consider mixing high CBD with high THC.
Other cannabinoids and hat may be useful for seizure control:
CBDV has been investigated as an anti-convulsant
- appears to have an additive effect when added to CBD
THCa, the non-psychoactive precursor to THC, is now available in CA in a measured oil.
- potent anti-inflammatory
- anecdotally it's an anti-convulsant
She has patients who can't get seizure control with CBD, so they added in THCa and have seizure control. She has patients that didn't respond to CBD but did to THCa.
CBN - conflicting reports
Delta-8 THC there's some tolerance that develops
THCV appears to be effective, but isn't readily available.
51:00 She shared a study she did with 200 of her patients that'd been on one cannabis oil for three months min.
- average # of drugs coming in was 12, ranging from 2 to 22
- After adding CBD the meds fell to an average of 3, with a range of 0 to 7.
- Patients present a wide range of other conditions. It's not just epilepsy they treat.
About 4% of patients had worsening seizures. It's hard to know if that was from drug interaction. Two of the 8 affected weren't on any medication.
About 6 patients had no response at all.
28 patients (14%) had no decrease in seizure events, but parents reported less intensity and shorter duration. When you're having a 2-minute seizure it feels like 20 minutes, so being able to get them down to something like 14 seconds is a change the families were happy with.
- They also reported cognitive improvement. The children were more alert and interactive.
Breaking down the seizures:
Overall they saw a 25 - 49% reduction in seizures.
18% had 50 -74% reduction
37% had 75 - 99% reduction
13% had seizure freedom
Over 68% of her patients surveyed had greater than 50% reduction in seizures.
Of the 27 seizure-free patients, 8 are off other medications.
- 40% were able to wean off one or more medications
The only side effects noted were drowsiness and diarrhea.
Diarrhea is a potential complication of too high a dose of CBD.
Positive side effects:
- more alert
- better mood
- better sleep
- more energy
- better responsiveness to therapy
- improved appetite
- improved focus
- less hospital stays
- less need for rescue medications
Two patients with diabetes reported a more stable glucose level when they added CBD to the regimen.
They start patients at 1 mg/kg per day. She doesn't like to start high because this is a huge expense out-of-pocket for the parents and some children respond to the low dose. If you start too high you miss the optimal therapeutic dose.
She increases every couple weeks, as long as the child is tolerating the dose. Doses are administered sub-lingual lay, orally, or through the g-tube.
Average dose if 5-10 mg/kg per day, but that's deceptive, because every patient is individual, and the doses were all over the place.
For non-responsive you can
- change the chemovar
- change the CBD:THC ratio
There appears to be no tolerance to CBD. Once you find the dose, it seems to stay consistent. Influences to a dose increase would be growing, gaining weight, or some other variable.
- When weaning off other drugs she may increase CBD, to drop the dose back down after the drug has been cleared from the system.
You want to stay consistent with the chemovar. With pediatric patients there's a real concern that switching chemovars can trigger an increase in seizure occurance and severity.
CBD Saturation: There's no research data to back this up, but it's being reported by clinicians. If a patient has been on a very high dose of CBD long-term (6 months to a year) there may be an uptick in seizures when there's nothing else to point the finger at.
- The solution: skip a half-dozen doses, anywhere from 1-3 days worth of doses, and then reset at a lower dose. The child typically does great.
Of 25-30 patients she's tried this with, only 1 didn't respond positively.
She sees a fair number of children with autism. Their concerns include
- communication
-repetitive behavior
- social challenges: anxiety, tantrums
- self-injurious behavior or harm to others
The ECS regulates emotional responses. Anxiety, behavioral, social interactions, immune system concerns are all aspects of autism.
It's been suggested that it's tied to genetic malfunction of the ECS. Children with autism had an abnormality in the number of eCB receptors expressed on their white blood cells.
There are many anecdotal reports of children with autism responding to CBD and THC, sometimes in combination.
She surveyed 27 patients. All started on high CBD:THC.
- About 15% got more agitated. CBD can be too stimulating for some patients. In low doses, CBD can be alerting. Higher doses can be sedating.
- 63% reported calmer behavior, reduction in self injury, improved communication, improved focus, improved reports from therapists and teachers.
Many of her parents don't tell teachers or therapists that the child is on a cannabinoid therapy, in the hopes of getting unbiased positive feedback from professional support teams.
Dosing is lower than for epileptic patients.
1 - 3 times a day
Popular strains to treat autism:
Harlequin, Cannatonic, AC/DC, Charlotte's Web,
High CBD to THC can be too stimulating. By lowering the ratio you can sometimes balance it out
Case study of a patient, a 10-yr old girl, that stopped wandering the house at night when they introduced a low dose of THC at night. She also had less anxiety and more focus and her sleep improved.
- on the weekends they began toggling the THC into the mix until they found the sweet spot.
5 mg of CBD + 3 mg THC resulted in
Low behaviors
Low anxiety
Less fixating
Teachers reported good days and good behavior
No signs of psychoactivity.
Pediatric cancer
Cannabis can be used to treat symptoms, but it will also
- inhibit tumor growth
- cause apoptosis
- inhibit metastasis
- inhibit angiogenesis
- recent evidence shows synergism with some chemo drugs
She uses combination high CBD and THC doses for cancer patients. It's all new territory with no real research to back it up yet.
She shared a story of a patient who came to her at 17 after years of chemo and numerous surgeries. They'd sent him home, telling him he had 90 days. The parents decided to go with cannabis and without her knowledge got him up to a gram a day, 1:1 CBD:THC. When the scans were done months later he was cancer-free.
Why do we persist in this madness? His oncologist sent him to Bonnie for end-of-life, after they'd put him through hell for years, right there in a state that was legal. Why do we allow this to persist? 

 I couldn't be happier to help you gain more understanding of how marvelously your body works and how powerful the healing force within you is.
I couldn't be happier to help you gain more understanding of how marvelously your body works and how powerful the healing force within you is. 
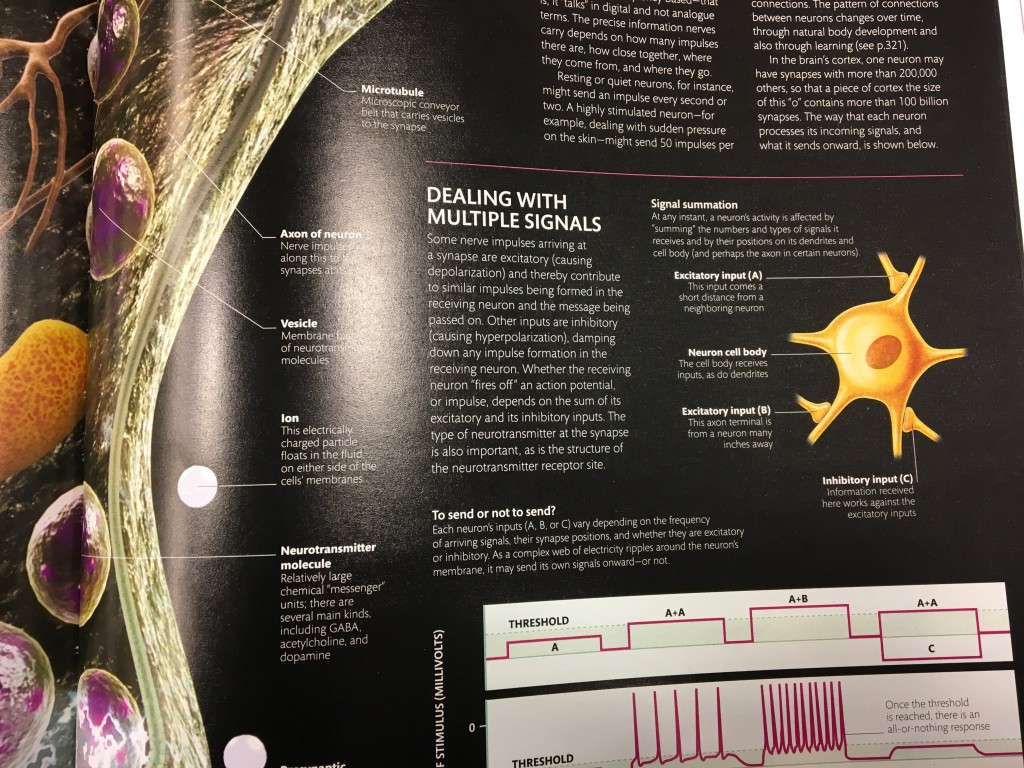
 "So having this auto-protective, negative feedback mechanism...so this is very different to how typical neurotransmitters work.
"So having this auto-protective, negative feedback mechanism...so this is very different to how typical neurotransmitters work.