

The journey begins..........
I came to 420 Magazine on a fit of whimsy. My husband was dying and I wanted to keep him high until the end. Since I was going to grow, why not do a grow journal? My only intent was to document the grow for my own record. After all, who cared what a 61-year old woman from the banks of the Monongahela had to say?
 I'm still adjusting to having become SweetSue. Lol!
I'm still adjusting to having become SweetSue. Lol! Well, my husband died the following year. Right at the end I discovered Concentrated Cannabis Oil (CCO). Of course, too late to be of any use to my beloved. The frustration of realizing the high price we'd paid for prohibition lit a fire that apparently is unquenchible. I'm driven to learn everything I can about how disease gets a foothold in our bodies and how we can use CCO to tip the scales in our favor and then to help us maintain the state of homeostasis we were evolved to experience. I switched my grow focus from strongly recreational to strongly medicinal. I'm making oil for my own use. Although I'm a healthy woman who takes no medication other than cannabis, I realize the benefit my own body can gain from including CCO in my life. I also accept that I'll be helping others in their own quest to make and administer CCO for healing and I can't very well do that without practical experience, can I?
This is no easy path, but I know we can make it fun. I study like a fiend, and this thread is my new study hall. It's my hope that some of you will decide to join me on my quest to not only master understanding of the diverse fields of knowledge I'm jumping into, but to help me break it down into simple terms and possibly illustrate it, so that what we end up with is a genuine resource that can help calm the desperation of a member looking for hope.
In the end we can take the mish-mash of what we developed and put it all together in an orderly fashion. Do our own handbook on achieving homeostasis using CCO. How's that sound?
I have this habit of wanting it all.
 I'm not certain what we'll end up with here, but I'm excited about the possibilities. I've broken it down into simple categories and I'm beginning with questions I personally want answers to. Some of this I already know, so it's a matter of composing the right answer and making it look like something you want to read. I have a concern that we have many members who learn more visually, so that has to be taken into consideration with anything we put together. I'm not interested in working in any particular order. My brain works more fluidly than that. I'll accept the responsibility of keeping track of what gets developed. My hope in putting this out there is that some of you will have an interest spark in one subject and find yourself compelled to master it so you can explain it to us. This doesn't have to be all SweetSue developed material. I have no ego. Please, contribute.
I'm not certain what we'll end up with here, but I'm excited about the possibilities. I've broken it down into simple categories and I'm beginning with questions I personally want answers to. Some of this I already know, so it's a matter of composing the right answer and making it look like something you want to read. I have a concern that we have many members who learn more visually, so that has to be taken into consideration with anything we put together. I'm not interested in working in any particular order. My brain works more fluidly than that. I'll accept the responsibility of keeping track of what gets developed. My hope in putting this out there is that some of you will have an interest spark in one subject and find yourself compelled to master it so you can explain it to us. This doesn't have to be all SweetSue developed material. I have no ego. Please, contribute. This is a community project, if you'll join me. I have no care for any credit. I have a great desire to continue developing materials that explain all this in simple terms. That's my only purpose in being here. Anybody game?
This is long-term work. I'm not expecting this to fly. We have lives that are worth being a part of and this search will plod along. I may study hard, but I play hard too.
Balance in all things. I want to be certain at every step that we got it right. There's a focus on cancer here because the cancer-killing potential of phytocannabinoids demands it. That does not mean we're limited to discussing using CCO to treat cancer. I'm also associated with cajuncelt's cancer protocol thread and I'm working on some materials for him as well. I figured toss it all out there, see what sticks. My starting questions. If anyone has some they'd like to add let me know within the next 420 minutes and I can edit them in.
A Rudimentary Understanding of Cellular Biology and Cancer Progression
- What's the life cycle of a healthy cell?
- How does programmed cell death happen?
- What's the difference between apoptosis (cellular suicide) and necrosis (cellular death)?
- What changes occur when a cell becomes cancerous?
- What are the stages of cancer?
- What's this about Demethylation?
Your Endocannabinoid System and Homeostasis
- What's the job of the Endocannabinoid System?
- How do receptors work?
- How can I assist my Endocannabinoid System?
How Cannabinoids Kill Cancer Cells
- apoptopic (apoptosis; cell seeks its own death)
- antiangiogenesis (keeps cell from growing new blood vessels)
- antiproliferative (keeps cells from reproducing)
- antimetastatic (cell can't spread seed)
- How does THC kill cancer cells?
- What special cancer-killing properties does CBD have?
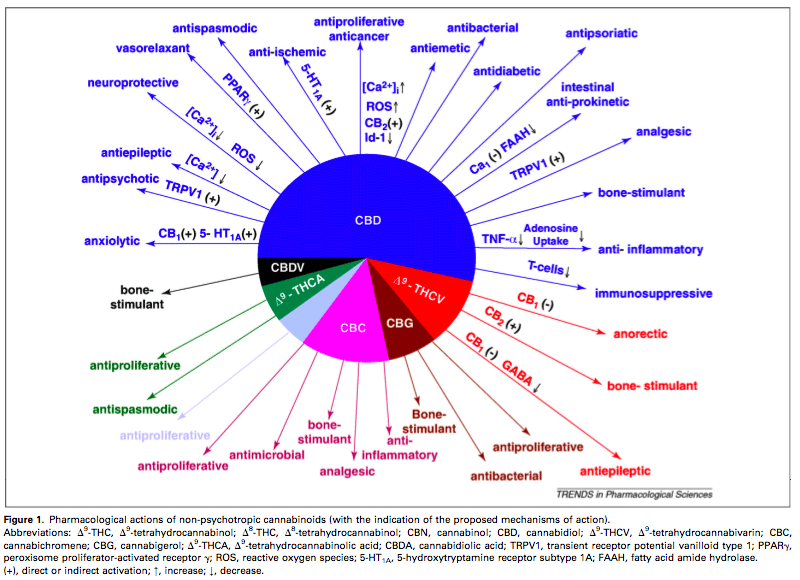
The Phytocannabinoids : Your Reserve Soldiers
- description of individual cannabinoids and terpenes)
Concentrated Cannabis Oil (CCO): The Great Equalizer
- Can I get stronger medicine if I use the whole plant?
- What's the easiest way I can find to make good-quality oil in my kitchen?
- What equipment changes will I need to make for producing a larger batch?
- Is there any way to reclaim at least some of the solvent?
- Can we get a decent hand on the truth and science behind decarboxylation?
- What technique gives me the highest THC numbers? CBD numbers?
- Which approach gives me the most monoterpenes?
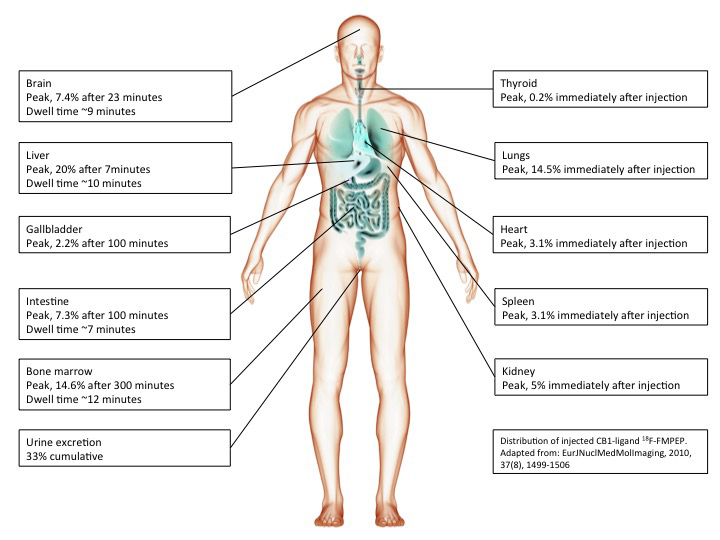
Supercharging The Oil: The Science of Bioavailibility
- Don't the cannabinoids just get in there and go to work killing diseased cells?
- How can I use the science behind liposomal encapsulation to my advantage?
- What's a carrier oil?
- Why are phenolic oils so important?
- What difference does the choice of carrier oil make?
- What's a Bio Bomb?
- How does Competitive Inhibition work?
- How do I incorporate Competitive Inhibition into the protocol?
Strains and Ratios: Customizing Your Medication
- Does it really make a difference which strains I choose?
- How does synergy come into play when I'm mixing the strains?
- What are recommended ratios for oil production?
- How would I work out using whole plant and mixing strains?
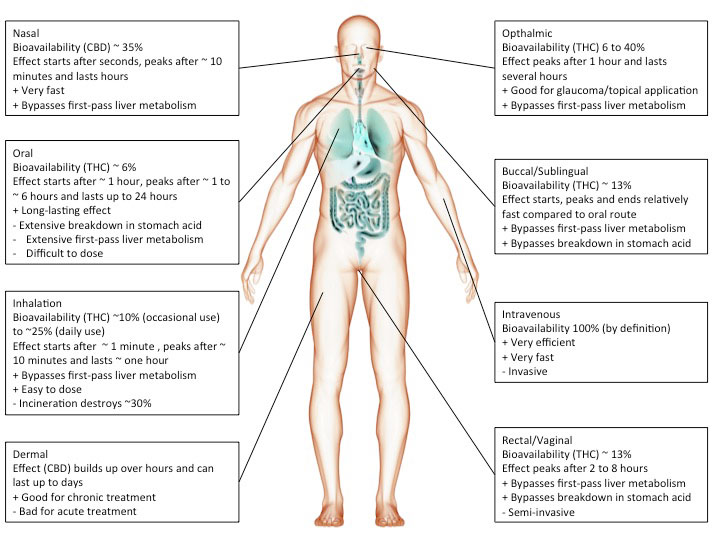
Dosing Protocols and Delivery Systems: Proceed With Care
- What are the pathways into the system and how effective are they?
- What do we mean by "First Pass"?
- What's "herxing"
- What's the difference between optimal dose and therapeutic dose?
- How would I determine a therapeutic dose?
- What level dose is a good starting point?
- How do you make a metered dose?
- How often should I be dosing?
- Explain "Start Low and Go Slow".
Resources For Patients: Boots On The Ground
- What patient support organizations exist?
- What kind of support system should I pull together?
Complementary Therapies
- What are some other holistic ways I can help my body gain homeostasis?
- How can breath training benefit me?
- What are some practical ways to stay positive?
Reading and Resource Lists
Random Notes
**********
I anticipate discussion and debate on occasion. My expectation is that the vision, the desire, the sheer joy we derive from the search for understanding will keep those debates civil.
 Make yourselves comfortable.
Make yourselves comfortable.



 I shall be studying this over and over. You're a legend...
I shall be studying this over and over. You're a legend...
