

SweetSue;3156027 said:This was too delicious a find to leave behind. It was written by a poster going by the name in vivo. I found it on the Michigan Medical Marijuana site. I didn't link any of the references. This was just an opportunistic find that found me.Enjoy.
"Posted 18 March 2014 - 04:36 PM
Cannabinoids display 'antitumor properties such as inhibition of cancer cell growth, induction of apoptosis and blocking the processes involved in tumor progression, such as angiogenesis, and cell migration. These effects might involve several signaling pathways being both cannabinoid receptor-dependent or independent' (Pisanti 2009).
When a person reads the above quote they may feel it's the end of the story. Cannabis kills cancer. But is that really where the story ends? Pro-cannabis researchers and pro-cannabis activists seem to have differing opinions on the answer. Many activists are promoting cannabis that's high in THC for any and all types of tumors. Researchers suggest that THC appears to have a great deal of potential in the treatment of a large number of cancer cell lines, but that it's not always the best cannabinoid to choose for a cancer based treatment. Why is that?
The level of expression (the number of) of cannabinoid receptors (CBRs) in tumor cells appears to be a fundamental factor to the overall effectiveness of cannabinoid based cancer treatments. Most cannabinoids are CBR activators. These CBRs are 'doing all the work' so to speak. It is not the cannabis or cannabinoids themselves that have anticancer properties, it is the cannabinoids ability to latch onto and activate the appropriate receptors. The activation of these receptors unleashes a cascade of events and mechanisms, some of which are advantages in slowing the progression and inducing apoptosis in tumor cells. CBR activation is fundamental to all cannabinoid based treatments. If this sounds relatively straight forward, that's because in a way it is. In order for cannabinoids to elicit any anticancer effects they must be able to activate the specific CBRs in the tumor cells. The higher the expression level of receptors, the greater impact that cannabinoids that activate those receptors have in the treatment. If there are no receptors to activate in the target area, or the cannabinoids being used are more effective at activating a different receptor, the treatment is likely to be relatively unsuccessful. (Pisanti 2009)
Equally vital is the awareness that tumor cells with low or undetectable expression levels of CBRs are resistant to any anticancer effects that cannabinoids may elicit, and the immunosuppression resulting from the systemic application of cannabinoids have been shown to enhance tumor growth in some cancer cell lines (like some types of breast cancer). (Pisanti 2009)
This paper will attempt to point to some of the research in relation to cancer, the endocannabinoid system (ECS), and natural cannabinoids that activate it. It may surprise some readers to learn that there is a growing number of legal and natural cannabinoids which originate outside of the cannabis plant. Many of these are cheap, highly available, and share a number of anticancer characteristics to cannabinoids in cannabis via the activation of similar receptors.
The primary targets or mechanisms of action in cannabinoid based cancer treatments involve the activation of CB1 and CB2 receptors. It seems likely that one reason THC has proven to be relatively effective (particularly when combined with other cannabinoids) is based on the fact that it's a CB1 and CB2 activator. However, THC activates CB1 much more efficiently than CB2, which is why other cannabinoids might be better options for treatments that would benefit from CB2 activation.
In addition to the activation of CB1 and CB2, some cannabinoids also activate TRPV1 which has been shown to induce apoptosis in tumor cells. Another target worthy of mention is GPR55. Unlike the other receptors which we are attempting to activate in cancer treatments, GPR55 activation by natural compounds in the body (as well as exogenous sources) actually leads to the proliferation of tumor cells, so it is beneficial to block GPR55 rather than activate it. Luckily enough there are cannabinoids that block GPR55. Both CBD and magnolia officinalis extracts block the activation of GPR55 and slow the proliferation of tumor cells. (Pisanti 2009)
Here is a list of cannabinoids with some of the relevant receptors that they target:
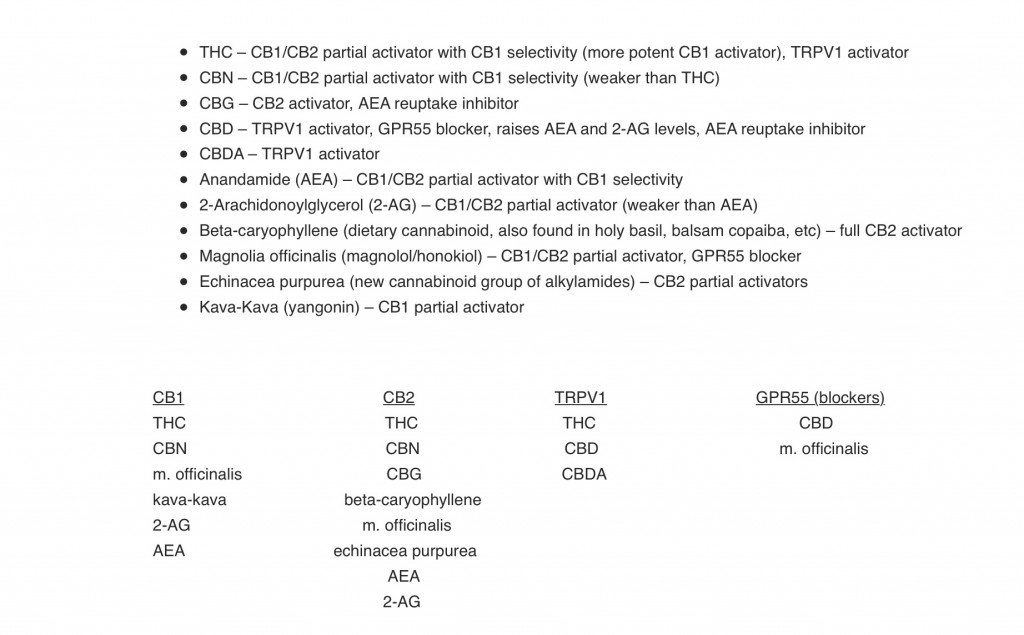
This is not a definitive list, but there might be a few cannabinoids listed that many patients aren't familiar with.
The first two I'll point out are AEA and 2-AG. These are endocannabinoids (natural cannabinoids in the human body). These are listed for a few select reasons. They are CBR activators with anticancer characteristics that are naturally produced by the body. That knowledge on its own might not mean much, but coupled with the knowledge of inexpensive ways of increasing endocannabinoid levels it can be quite useful information. Dietary linoleic acid has been shown to raise levels of both AEA and 2-AG. This is an inexpensive way to increase the body's own natural cannabinoids. CBD also raises levels of both AEA and 2-AG via FAAH inhibition. In addition, CBD, CBG, and CBC are all AEA reuptake inhibitors (which raise AEA levels).
Next is beta-caryophyllene. Beta-caryophyllene is of value in that it is a full CB2 activator that is naturally found in a number of dietary sources. It can also be found in concentrated levels in a variety of essential oils and nutritional supplements. In some treatments (like some types of breast cancer) CB2 activation is likely of greater importance than CB1.
One of the most highly researched in regards to anticancer potential is the magnolia officinalis. Magnolia officinalis root bark has been used in Chinese medicine for 2000 years. It contains magnolol and honokiol which are both cannabinoids with anticancer characteristics. They activate CB1, CB2, and also block GPR55. A point worth mentioning is that they are both known to target apoptosis, which might make their addition to any cannabis based (specifically THC) treatment potentially beneficial.
The final two are echinacea purpurea (CB2 activator) and kava-kava (CB1 activator). These are both relatively new discoveries and there isn't much information about their specific characteristics in regards to cancer treatment, but as CB1 and CB2 are both targets, it might be safe to assume that these have potential as well.
So now that we are familiar with our targets (receptors) and our weapons (cannabinoids) let's see how this all relates to some types of cancer:
Breast Cancer
CB1 expression level is lowered
CB2 expression level rises
AEA and 2-AG via CB1 activation reduces cell proliferation
THC immunosupression and non CBR mechanisms have been shown to increase tumor growth and metastisis in some cell lines.
THC induces apoptosis via CB2 activation (better options for CB2 activation)
CBD inhibition and apoptosis via CB2 and TRPV1
Magnolia officinalis cannabinoids have a great deal of positive research in this treatment
THC might not be the most appropriate cannabinoid for this treatment. (Reader is advised to review research on individual cancer cell lines in relation to this topic in the provided citations.)
Prostate Cancer
CB1 and CB2 expression levels rise
TRPV1 expression levels rise
AEA via CB1 and CB2 inhibits proliferation
THC induces apoptosis via non CBR
Other cannabinoids have been shown to induce apoptosis via CB1 and CB2
Magnolia officinalis cannabinoids have a great deal of positive research in this treatment
Many cannabinoids might be well suited
Skin cancer
No information on changes of expression levels, but CB2 is highly expressed in the skin
Cannabinoids have been shown to inhibit growth via CB1 and CB2 activation
Beta-caryophyllene from essential oils can be used in topical applications
Magnolia officinalis cannabinoids have a great deal of positive research in this treatment
Pancreatic Cancer
CB1 and CB2 expression levels rise
THC induces apoptosis via CB2 and ceramide
Magnolia officinalis cannabinoids have a great deal of positive research in this treatment
Many cannabinoids may be well suited
Glioma and Brain Cancer
CB2 expression levels rise (CB1 level of expression in brain is high)
THC induces apoptosis via CB1 and CB2
THC reduces proliferation via CB1
THC inhibits cell invasion via non CBR mechanisms
Other cannabinoids have been shown to induce apoptosis via CB2 and COX-2 inhibition
Magnolia officinalis cannabinoids have a great deal of positive research in this treatment
THC is prime candidate
GI/Colon Cancer
CB1 expression levels rise in gastrocarcinoma
CB2 expression levels rise in colon carcinoma
AEA induces cell death via COX-2 (colorectal carcinoma)
AEA synergism with 5-fluorouracil
Other cannabinoids inhibition via non CBR mechanisms
Other cannabinoids induce apoptosis via CB1 and CB2
Magnolia officinalis cannabinoids have a great deal of positive research in this treatment
Loss of CB1 accelerates intestinal tumor growth
Hematological Cancer
CB2 expression levels possibly rise
AEA induces apoptosis via TRPV1 (other TRPV1 agonists)
AEA growth inhibition and apoptosis via CB1 and CB2
THC induces apoptosis via CB2
CBD growth inhibition and apoptosis via non CBR
It also seems important to stress the potential relevance of treatment schedules. This is a point that directly relates to the expression level of CBRs, which we now understand the role of. The average lifespan of a cannabinoid receptor is around 0.5 seconds. Their level of expression is constantly in flux. Patients who have consumed cannabis for extended periods of time are familiar with the fact that a "tolerance" is quickly established to cannabinoids. The same is true for patients during cancer treatments. This is in large part due to the level of cannabinoid receptors being lowered and becoming fatigued by the constant exposure to exogenous cannabinoids. It is also commonly accepted among those who consume cannabis daily that abstaining from cannabis for 24-48hrs lowers a person's tolerance and increases the effects elicited by cannabinoids.
How does this relate to cancer treatments? Well, some research suggests that the efficacy of a cannabinoid based treatment is influenced by the dosing schedule. Most cancer treatments recommend 1000mg of cannabinoids daily. Is that the most effective schedule? Is it possible that incorporating 'off days' and abstaining from cannabinoids might allow the CBRs to recover and increase the efficacy of the overall treatment? Scientific research indicates this to be the case. (Scott 2013)
Due to the reduction of receptor expression levels as well as receptor fatigue from overexposure to CBR activators, it has been shown that it might be significantly more effective to incorporate a 'day off' every fourth day in which no cannabinoids are consumed. This allows the expression levels of CBRs to rise and allows them to recover from fatigue, in turn this has been shown to increase the efficacy of subsequent cannabinoid applications. This might be something worth considering for those involved with these types of treatments. (Scott 2013)
This paper isn't meant to be definitive, but I hope it provides patients with some potentially useful insight into cannabinoid based cancer treatments. The ways in which we discuss the potential of cannabinoids have a direct impact on current treatments. When a claim is made that 'cannabis cures cancer' that statement taken at face value is potentially dangerous in some scenarios. Cannabis doesn't kill cancer in the traditional sense, or similar to the way that chemotherapy does. Chemotherapy targets and kills practically everything. That is one reason why cannabinoids offer so much more potential in cancer treatments. Cannabinoids, some of which can be found in cannabis, can be used to coax the body into slowing these cells down and convincing them to kill themselves in a nontoxic way. But it's important to know how to use them by understanding which ones to use. This is gained by identifying the specific receptors that are being targeted. Once the targets have been identified a combination of activators can be utilized to activate those targets. This message is lost when we speak about the use of cannabis in cancer treatments in an inappropriate manner. Just talking about this more accurately might increase awareness which might have the potential to increase the efficacy of current cannabinoid based treatments.
It is highly recommended to review some of the citations (available online for free) as they provide much more detailed information.
References:
Guindon, Josée, and Andrea G. Hohmann. "The endocannabinoid system and cancer: therapeutic implication." British journal of pharmacology 163.7 (2011): 1447-1463.
Pisanti, Simona, and Maurizio Bifulco. "Endocannabinoid system modulation in cancer biology and therapy." Pharmacological Research 60.2 (2009): 107-116.
Alvheim, Anita R., et al. "Dietary Linoleic Acid Elevates Endogenous 2AG and Anandamide and Induces Obesity." Obesity 20.10 (2012): 1984-1994.
Ligresti, Alessia, et al. "Kavalactones and the endocannabinoid system: The plant-derived yangonin is a novel CB< sub> 1</sub> receptor ligand." Pharmacological Research 66.2 (2012): 163-169.
Amiel, Eitan, et al. "-Caryophyllene, a compound isolated from the biblical balm of gilead (Commiphora gileadensis), is a selective apoptosis inducer for tumor cell lines." Evidence-based complementary and alternative medicine 2012 (2012).
Gertsch, Jürg, et al. "Beta-caryophyllene is a dietary cannabinoid." Proceedings of the National Academy of Sciences 105.26 (2008): 9099-9104.
Fried, Levi E., and Jack L. Arbiser. "Honokiol, a multifunctional antiangiogenic and antitumor agent." Antioxidants & redox signaling 11.5 (2009): 1139-1148.
Seo, Jae-Uk, et al. "Anticancer potential of magnolol for lung cancer treatment." Archives of pharmacal research 34.4 (2011): 625-633.
Xu, Huanli, et al. "Targeting apoptosis pathways in cancer with magnolol and honokiol, bioactive constituents of the bark of Magnolia officinalis." Drug discoveries & therapeutics 5.5 (2011).
Rempel, Viktor, et al. "Magnolia Extract, Magnolol, and Metabolites: Activation of Cannabinoid CB2 Receptors and Blockade of the Related GPR55." ACS Medicinal Chemistry Letters 4.1 (2012): 41-45.
Izzo, Angelo A., et al. "Inhibitory effect of cannabichromene, a major nonpsychotropic cannabinoid extracted from Cannabis sativa, on inflammation induced hypermotility in mice." British journal of pharmacology 166.4 (2012): 1444-1460.
Scott, Katherine Ann, et al. "Enhancing the Activity of Cannabidiol and Other Cannabinoids In Vitro Through Modifications to Drug Combinations and Treatment Schedules." Anticancer research 33.10 (2013): 4373-4380.
Edited by in vivo, 18 March 2014 - 06:33 PM."
SweetSue's Cannabis Oil Study Hall
- Author AKgramma
- Create date
Blog entry information
More entries in Member Blogs
-
 Is Cannabis Market Transforming into a Fast-Moving Consumer Goods (FMCG) Sector?Traditionally, the global cannabis consumption market was viewed mainly as a raw material...
Is Cannabis Market Transforming into a Fast-Moving Consumer Goods (FMCG) Sector?Traditionally, the global cannabis consumption market was viewed mainly as a raw material... -
The Rise of Skate Vape: A New Design Trend in Cannabis ConsumptionAs the cannabis vaping market continues to evolve, new product trends are emerging that push the...
-
Why the Vape with Screen is Gaining Popularity in Cannabis?The cannabis vaporizer industry is evolving rapidly, and one trend that has gained significant...
-
How to Choose the Right Cannabis Vape with A Screen for YouAs the cannabis industry rapidly evolves, the competition among suppliers has intensified...
-
Why Are More Cannabis Brands Introducing Vapes with Screen Display?As the cannabis industry rapidly evolves, the competition among suppliers has intensified...